By
Julie Wassmer and Candy Gregory
Why is the UK government ignoring Pfizer’s own advice on second dosing?

Julie Wassmer writes…
Back in November, Health Secretary Matt Hancock announced to Parliament that the NHS was “to inject hope into millions of arms”.
He was, of course, referring to the development of vaccines to fight Covid-19 and an ambitious UK government plan to vaccinate as many people as possible as quickly as possible.
The government’s website describes this as “the largest vaccination programme in British history”.
During a recent Downing Street press conference, Hancock went on to announce: “We’re on track to deliver our plan to vaccinate the most vulnerable groups by the middle of February, the groups that account for 88% of Covid deaths. Our approach is, of course, to save as many lives as possible – as quickly as possible and to reduce the pressure on the NHS.”
Hancock also stressed the “Prime Minister’s target of offering vaccines to the top four priority groups by the middle of February”.
That target followed the recommendations for priority set by the Joint Committee on Vaccination and Immunisation (JCVI) – the UK body advising the government on vaccination, which claims there is “currently no strong evidence to expect that the immune response from the Pfizer-BioNTech and AstraZeneca vaccines differ substantially from each other.”
But in fact, the two vaccines differ substantially from each other in fundamental ways.
How vaccines work
Vaccines function by provoking the body to recognise and respond to proteins produced by organisms such as a virus or bacteria. Traditional vaccines are composed of inactivated doses of the organism or proteins that it produces, which are then injected into the body so that the immune system is prompted to mount a response.
However, the Pfizer vaccine (and the Moderna, which has recently been approved for use) are what are known as RNA vaccines and follow a new technology: by injecting a fragment of the virus’s genetic code into the body, which then produces part of the virus to which the body mounts a defence. The Pfizer vaccine has been approved for use in the UK, Europe and the US. The Moderna vaccine has also been approved but is not expected to become available for use in the UK until the spring.
The Oxford/AstraZeneca vaccine differs in that it uses a harmless virus to carry the same genetic material into the body. This has been approved in the UK and Europe. Of the three vaccines, the Oxford/AstraZeneca is the easiest to use as it can be stored in a fridge rather than needing very cold temperatures, as shown on the following chart.
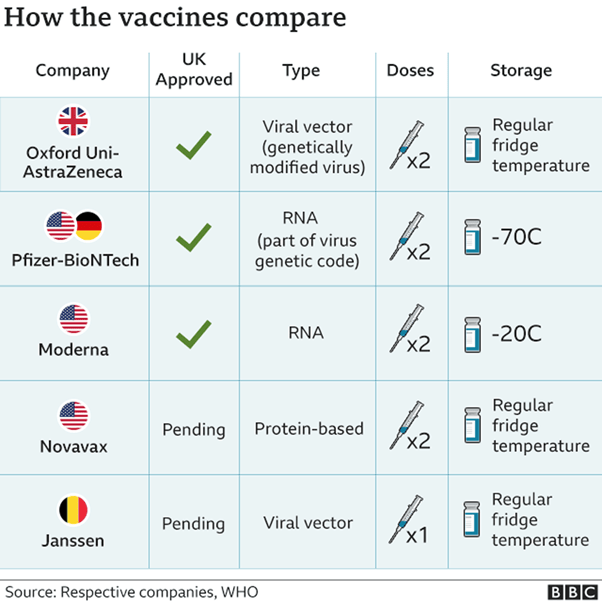
A crucial point is that the Pfizer, Moderna and Oxford/AstraZeneca vaccines should be administered in TWO doses.
Pfizer stipulates that their vaccine should be given 21 days after the first, while the Oxford/AstraZeneca vaccine can be safely given as late as 12 weeks after the first. In fact, AstraZeneca states that its data showed an “8 to 12 week gap” was a “sweet spot” for efficacy.
However, on December 30, the UK government suddenly determined that second doses of both the vaccines currently available (Pfizer and Oxford/AstraZeneca) should be made no sooner than 12 weeks.
This followed a decision by the JCVI, which, while admitting the second vaccine dose is “important to provide longer lasting protection,” believes it expects the second dose to be “as or more effective when delivered at an interval of 12 weeks from the first dose.”
“Like going into the Wild West”
This bold decision caused considerable shock and concern across the world because, as both the World Health Organisation (WHO) and Pfizer have reminded the UK government, there is actually no data to support protection being afforded for the Pfizer vaccine when given as late as 12 weeks.
Dr Anthony S.Fauci, the leading US infectious disease expert, told CNN he would not be in favour of “delaying the administration of second doses” while Dr Eric Topol of the Scripps Research Translational Institute in California, tweeted: “That’s good because that is following what we know, the trial data with extraordinary 95 per cent efficacy, avoiding extrapolation and the unknowns.”
The decision by the JCVI itself is clearly an “extrapolation” of the Pfizer data because such delays have never been tested in Pfizer’s trials to support the 95% effectiveness figure beyond second doses given later than three to four weeks after the first.
Dr Phyllis Tien, an infectious disease physician at the University of California, described “straying from this regimen” as “like going into the Wild West”, insisting that such a change in dosing “needs to be data driven.”
Extending the gap between the recommended doses of a vaccine risks reducing the power of the second dose, which is designed to boost immunity against the virus, thereby improving the effects of the first dose which could be waning at that time.
Regarding Pfizer’s vaccine, Natalie Dean, a biostatistician at the University of Florida, was reported as saying: “We don’t really know what happens when you only have one dose after, like, a month… It’s just not the way it was tested.”
The JCVI defended its support for delayed dosing, insisting that “initially vaccinating a greater number of people with a single dose will prevent more deaths and hospitalisations than vaccinating a smaller number of people with two doses”. However, the WHO’s own Sage group duly responded by backing Pfizer’s warning and recommending that the second Pfizer dose should only be delayed in “exceptional circumstances” and then for only up to six weeks.
Recently, the British Medical Association weighed in with its own members’ concerns, challenging the government over this policy. In a letter to Chris Whitty, the UK’s chief medical officer, they urged the government to reduce the gap between Pfizer doses to a maximum of six weeks.
Whitty claimed that the longer wait between doses was a “public health decision” aimed at vaccinating many more people and based on the fact that the great majority of protection comes from the first jab.
However, a BMA blog from five highly respected medical professionals recently asserted very comprehensively that the government’s policy is based on a “non-randomised, uncontrolled population experimental study without pilot data” and said that “the Joint Committee on Vaccination and Immunisation (JVCI) and Public Health England should be prepared to revisit and, if necessary, reverse their decisions based on emerging scientific evidence. At the time of writing a statement released by Israeli officials has indicated that “real world” analysis of 200,000 people age 60 years who have had the first dose of the Pfizer vaccine shows efficacy of 33%, far less than the 89% stated by the JCVI. These new real-world data suggest that the UK should reconsider the decision to delay the second dose of the Pfizer/BioNTech.”
Labour peer and veteran broadcaster Joan Bakewell has also tried to raise awareness of this issue with the threat of a legal challenge to the UK government’s policy. Bakewell received a first dose of Pfizer vaccine and was told she would get a second dose three weeks later, but says that other elderly people were left “in limbo” by the government’s subsequent decision for the second dosing at 12 weeks, and she is therefore seeking a judicial review on the grounds of:
– Breach of the conditions of authorisation for use of the drug agreed between Pfizer and the Medicines & Healthcare products Regulatory Agency.
– Unlawful departure from the MHRA’s assessment that the effectiveness of the drug has so far been demonstrated in evidence only for 21 days, or at most 28 days.
– Breach of patients’ legitimate expectation that they would receive a second dose after 21 days, undermining their informed consent to accept the first dose.
In spite of the weight of opposition to the government’s decision on this important issue, there has been no change in strategy; in fact, the government has become even more intransigent on the subject, threatening to withdraw hospitals’ licences to vaccinate if they dare to administer a second dose before 12 weeks.
All this, in spite of the existence of new cases of Covid-19 emerging among those who had received a first dose of vaccine up to a month before testing positive – including medical staff.
The UK currently has the highest death rate per capita in the world and has lagged behind so many other countries in instituting effective controls against this deadly pandemic. We were late in providing PPE for healthcare staff; in recognising the need for testing at airports; for the proper quarantining of visitors to the UK; for heeding the advice of teaching unions on the risks within educational establishments; for allowing tens of millions of people to travel and mix on Christmas Day — while knowing the new variant was rampant. But also, throughout last summer the government actively encouraged and financially sponsored citizens to enjoy meals out in pubs and restaurants. None of this made sense to other countries that had taken effective control of the virus and whose strategies could and should have stood as an example to us, and a road map out of the recent tragic and appalling milestone of more than 100,000 reported Covid-related deaths.
China began screening and quarantining arrivals from Wuhan, the centre of the coronavirus outbreak, from January 3 last year, and Hubei, the province in which Wuhan is situated, is now back to normal life. It has not seen a case of Covid-19 in seven months and had effectively controlled the virus with a rigid five-month lockdown supported by mass testing and contact tracing.
By the end of January 2020, South Korea had established no fewer than 288 screening clinics offering tests, as well as requiring arrivals from China to quarantine. All arrivals into South Korea, regardless of length of stay or nationality, were required to be tested and to undergo quarantine.
By last July, only 289 of South Korea’s 51 million inhabitants had died from the virus since its first case in February – compared with 44,600 Covid-19-related deaths among the UK’s 66 million population.
To date, deaths in South Korea from Covid-19 are still below 1,500 with the number of daily cases running at below 500.
The UK government was strongly, and rightly, criticised for acting too late over border policy, with the home affairs committee of MPs publishing a report in August, finding that a lack of measures earlier in the pandemic was a “serious mistake” and the change in rules in March (suggesting that any arrivals in the UK should only self-isolate if suffering symptoms) was “inexplicable”.
Even the Home Secretary, Priti Patel, is on record as stating the UK should have closed its borders in March 2020 in light of the pandemic.
There are numerous mistakes that could be cited in the UK — for instance sports events such as the Cheltenham Festival were allowed to go ahead in spring last year. Baroness Dido Harding, later to become the head of our Test, Track & Trace system (which was anything but world beating and will have cost the taxpayer £23 billion by March this year) was connected to the event by virtue of her Jockey Club status.
Boris Johnson’s own dismissive attitude to the virus led a poor example when he boasted that he shook hands with “everyone”, including Covid patients, and would continue to do so.
China dealt effectively with the virus by treating the pandemic as a state of emergency (on a par with a national-security issue) and concentrated on controlling the public health crisis ahead of concerns for the economy. The strategy paid off. The virus is controlled and the Chinese economy is now thriving. Here, the government’s strategies were tardy and hampered by its desire to “balance the economy”, so that, ultimately, there were failures all round.
Now we have a vaccination programme in which the government is putting all its faith, while encouraging us to do the same. That message appears to be effective, as the majority of UK citizens do welcome an invitation to accept a vaccination against Covid-19 – even though they may not know which vaccine they are accepting or whether it will be effective against the new variants.
The vaccine programme is being effectively managed by the NHS — but with Medacs (the private company of which Tory donor Lord Ashcroft is the main shareholder) having been given a contract for part of the rollout.
Thus far, according to supply, it’s a crap shoot as to whether we might receive the Pfizer or Oxford/AstraZeneca vaccine. Certainly my own medical centre has used both as first doses, and friends and family members who have received the Pfizer vaccine in January have been given a date for second dosing — in April.
The government is sticking rigidly to its JCVI advice in spite of all the warnings from WHO, Pfizer, the BMA, the recent Israeli findings of only 33% effectiveness after a first dose; the cases of Covid infection that have still occurred four weeks after first vaccinations and, most recently, opposition by the Doctors’ Association UK which gave its own warnings in a letter addressed to health bosses including Matt Hancock, Chris Whitty, vaccines minister Nadhim Zahawi and Sir Simon Stevens, chief executive of the NHS, stating: “We must be clear that it is completely unacceptable to ignore the need for a second vaccination.”
“All studies confirm the need for this to provide reliable and lasting immunity.”
Listening to a JCVI spokesman recently, I could hardly believe the conceit behind its decision in the face of all these warnings, describing the recent Israeli findings as only an “extrapolation” when clearly the JCVI’s decision is based on nothing more than an “extrapolation” of the Pfizer trial data.
Meanwhile, as the UK vaccination programme continues apace, with over seven million people having been vaccinated thus far, our government’s continual boasting of these figures underscores something very alarming for me: the fact that the number of “jabs in arms” seems to be more important than administering effective complete vaccinations.
Furthermore, it should be noted that if supply problems lead to the Pfizer vaccine becoming unavailable for a second dose — even at the late stage of 12 weeks — the mixing of different vaccines also has been strongly warned against. But could our government be planning to ignore such caveats too?
I’m reminded that only a year ago, this same government was discovered to be shamefully attempting to mask the inadequacy of its medical supplies by quoting the number of surgical gloves available as single items rather than pairs.
Should its obsession with numbers lead the UK to vaccinate a greater number of people ineffectively rather than a lower number properly, and to the manufacture’s guidelines, and should it continue to ignore all the warnings it has been given regarding the importance of dosing correctly, it could be adding to its list of failings on Covid-19 in perhaps the most dangerous way of all.
Candy Gregory writes…
When the MHRA {Medicines & Healthcare products Regulation Agency} approved vaccines for rollout across the nation, this was greeted with huge relief and seen as our exit route from the Covid-19 pandemic; none more so than the healthcare professionals who have fought on a daily basis to care for Covid patients. Their anger on social media was evident, with fingers pointed towards the inadequacy and corruption of the government who presided over the worse Covid death rate per capita in the world. The Covid deaths of over 100,000 and rising includes over 840 healthcare workers.
Medics and scientists reviewed the data from the universities and pharmaceutical companies. The evidence from the Pfizer’s vaccine had been trialled and approved for giving the second of the two doses no more than 21 days after the second. Pfizer’s research shows no evidence of what the efficacy of its vaccine will be after 21 days.
So while the country was celebrating a light at the end of the tunnel, NHS England took a decision to extend the dosage intervals from three weeks to 12 weeks.
The pretext was that getting one dose to more people would offer more population protection that the researched evidence of efficacy of the two doses at 21 days’ interval for a full vaccination. However, chief medical officers also believed there would be a vaccine shortage and saw this Plan B as an alternative.
This change of plan after the programme had already started created great turbulence and perplexity among medics. As a workforce that relies on evidence to care for the sick and vulnerable, there was great agitation and uncertainty. Was this Plan B for the good of their patients or the good of the government’s statistical bragging rights?
The BMA has called the government’s change to a 12-week interval “unreasonable and totally unfair” as they had no means of reassuring patients that the new JCVI guidelines were in their best interests but were compelled to “go with it” as there was no alternative.
There was also the matter of consent. Patients had consented to a three-week interval between doses and not a 12-week interval.
Medics were worried and patients were worried. Nowhere else is following suit, other than Ottawa in Canada — and only due to a dwindling supply of vaccine there. Others are simply observing how it affects our population. The UK seems to have been signed up to a clinical trial without consent. An unethical move and a massive gamble. The virus has already mutated and there is a theoretical risk that tampering with the dosage interval may allow for vaccine resistance.
But currently this is what the situation is: one dose, and then wait 12 weeks for possible full vaccination protection.
In the mean time, professional bodies are calling on the Health Secretary, Matt Hancock, to investigate the effects of delaying the second dose.
At present the best we can do is cross fingers and hope there is an acceptable rationale for their new but seemingly unproven vaccine regime.
As a nurse who is taking part in the vaccine programme, this change of policy doesn’t sit easily — but patients are now aware of the situation and we are all desperate for this pandemic to be a distant memory.
What you can do
You can help by donating to the legal challenge: https://www.crowdjustice.com/case/pfizer-vaccine-roll-out/
OR
You can help by signing this petition: https://www.change.org/p/2nd-covid-vaccine-should-be-21-28-days-not-12-weeks-challenge-u-k-government-petition-parliament-uk-petitions-566116
About
Julie Wassmer is a TV drama writer, author and environmental campaigner. www.juliewassmer.com
Candy Gregory is a founder member of Save Our NHS in Kent and a retired registered nurse who has rejoined the profession to help with the vaccine roll-out programme. She lives in Thanet, where she is an independent councillor on Thanet District Council.
Ways You Can Help Whitstable Views:
- Make sure you share and like our articles on Facebook and Twitter, and whatever other social-media platforms you use.
- Follow the site to get regular updates about new articles when they appear. Press the “Follow” icon in the bottom right hand corner of your screen and that will take you to the option to sign up. (It disappears as you move the text down, then reappears as you move it back up again!)
- Leave comments on the site rather than on Facebook. Let’s get a debate going. All of our contributors are willing to engage with you if you leave a comment.
- To all writers out there, we would LOVE you to make a contribution. Read our submissions page for details on how to go about that: https://whitstableviews.com/submissions/
- Finally you can donate. As little as £1 would help. Details on the donations page here: https://whitstableviews.com/donate/
